Beth S. Granet, Frank Golom, Ph.D.
The Impact of Medication Compliance and Cognitive Ability on Decisional Capacity Assessments of Patients with Psychotic Disorders
{kind=link}
Abstract
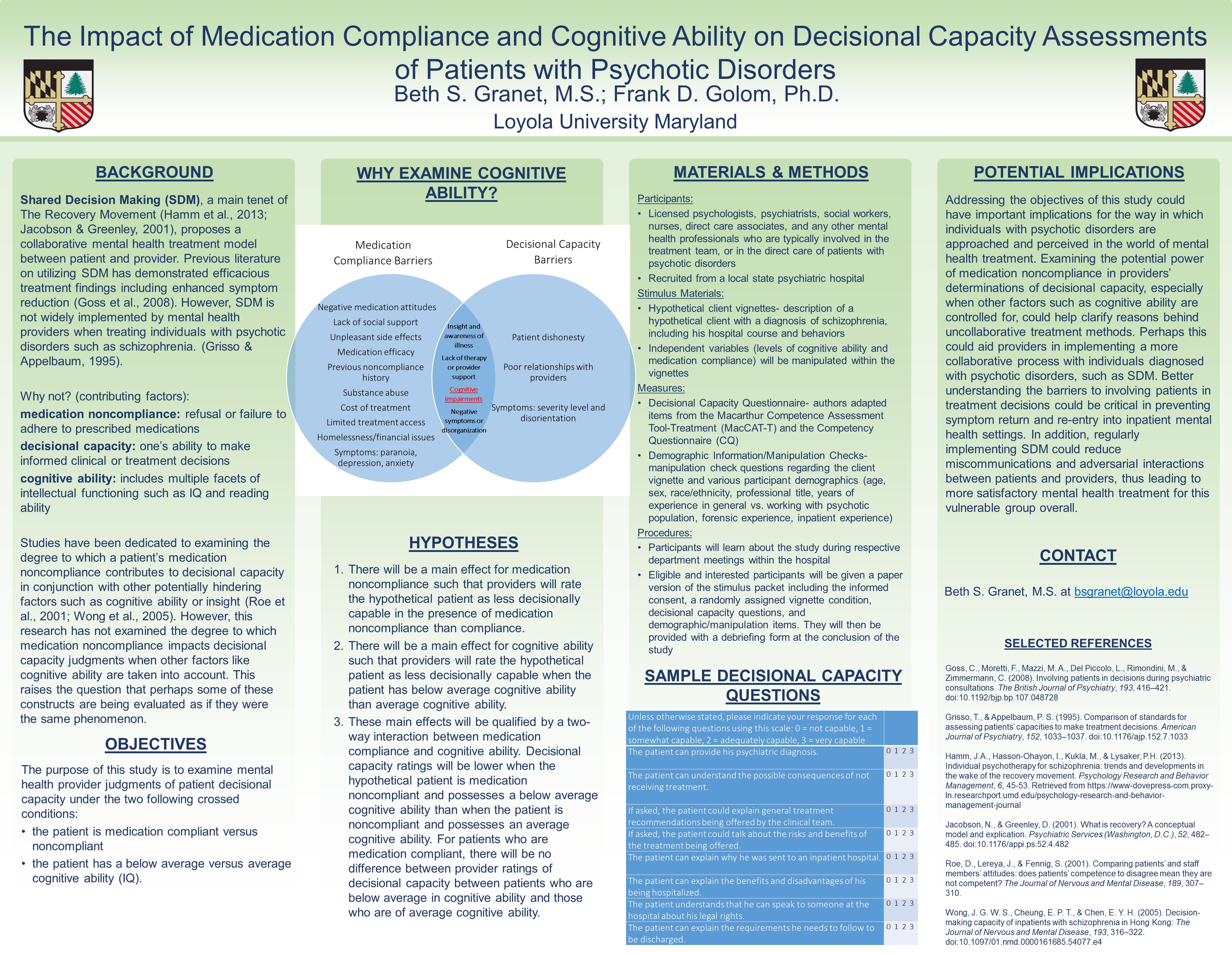
Shared Decision Making (SDM), a main tenet of The Recovery Movement (Hamm et al., 2013; Hasson-Ohayon et al., 2013; Jacobson & Greenley, 2001; Rose et al., 2011), proposes a collaborative mental health treatment model between patient and provider. The SDM approach during treatment planning designates both the patient and doctor as experts working together, allowing patients to relay subjective experiences, and receive an explanation of all treatment possibilities (Goss et al., 2008; Hamann et al., 2003; Hamm et al., 2013; Spaniol et al., 2002). Previous literature on utilizing SDM has demonstrated efficacious treatment findings including enhanced symptom reduction (Charles et al., 1997; Essock et al., 2003; Priebe et al., 2007; Stevenson et al., 2004; Swanson et al., 2007). However, SDM is not widely implemented by mental health providers when treating individuals with psychotic disorders such as schizophrenia, due to several potential client-related barriers (Grisso & Appelbaum, 1995; Hamann et al., 2003; Szmuckler, 1999). These barriers, including medication noncompliance, lack of decisional capacity, one’s ability to make informed clinical or treatment decisions, and impaired cognitive ability, also referred to as intellectual functioning or intelligence, overlap in the existing literature (Beck, 1987; Chong et al., 2013; Laugharne & Brown, 1998; Mandarelli et al., 2014; McKinnon, et al., 1989; Wong et al., 2005). More specifically, some studies have been dedicated to examining the degree to which a patient’s medication noncompliance contributes to decisional capacity in the context of other potentially hindering factors such as cognitive ability (Raffard et al., 2013; Roe et al., 2001; Wong et al., 2005). However, this research is void of a direct link between decisional capacity and medication compliance of a patient, especially while accounting for the factors contributing to each. This raises the question that perhaps some of these constructs are being evaluated as if they were the same phenomenon. Therefore, this study examines the potential effect of medication compliance on a provider’s judgment of patient decisional capacity during treatment planning and clinical decision making while explicitly accounting for a patient’s cognitive ability.
The purpose of this study is to examine mental health provider judgments of patient decisional capacity under the two following crossed conditions: the patient is medication compliant versus noncompliant, and the patient has a below average versus average cognitive ability (IQ). These conditions will be examined utilizing a sample of approximately 60-80 treatment providers from a local state psychiatric hospital. Various demographic variables such as age, sex, race/ethnicity, professional title, years of experience as a mental health provider, years treating a psychotic population, years working in an inpatient setting, and any forensic experience will be collected from each participant. Participants will be provided with a client vignettes detailing a hypothetical male patient diagnosed with schizophrenia, including information such as his hospital course and behaviors as well as his level of medication compliance and cognitive ability (IQ). Participants will be given a questionnaire on which to rate the decisional capacity of the hypothetical patient with varying degrees of medication compliance and cognitive ability.
The authors predict that there will be a main effect for medication noncompliance such that providers will rate the hypothetical patient as less decisionally capable in the presence of medication noncompliance than compliance. Additionally, there will be a main effect for cognitive ability such that providers will rate the hypothetical patient as less decisionally capable when the patient has below average cognitive ability than average cognitive ability. These main effects will be qualified by a two-way interaction between medication compliance and cognitive ability. Decisional capacity ratings will be lower when the hypothetical patient is medication noncompliant and possesses a below average cognitive ability than when the patient is noncompliant and possesses an average cognitive ability. For patients who are medication compliant, there will be no difference between provider ratings of decisional capacity between patients who are below average in cognitive ability and those who are of average cognitive ability. Addressing the above research purpose could have important implications on increasing the use of SDM with a psychotic population. Better understanding the barriers to involving patients in treatment decisions could be critical in preventing symptom return and re-entry into inpatient mental health settings. In addition, regularly implementing SDM could reduce miscommunications and adversarial interactions between patients and providers, thus leading to more satisfactory mental health treatment for this vulnerable group overall.
Keywords: shared decision making, schizophrenia, decisional capacity, recovery
Quick Details
Watch this space for more information about
the 15th annual Emerging Scholars event, planned
for April, 2026.