Kelly Rootes-Murdy, Marianna E. Carlucci, Ph.D., Irving Reti
Nonsuicidal Self-Injury on Electroconvulsive Therapy Outcomes in Adolescents and Young Adults
{kind=link}
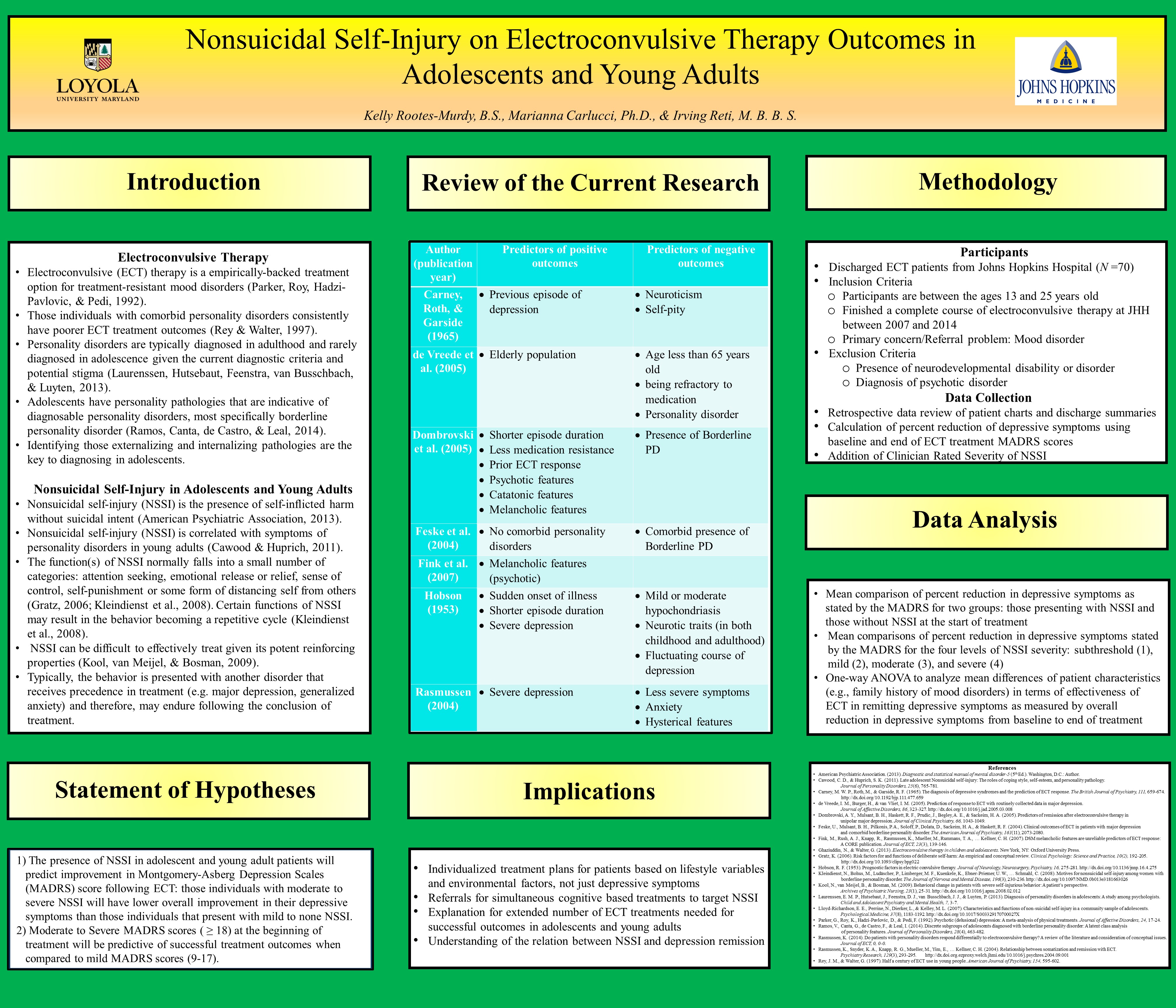
Electroconvulsive (ECT) therapy is an empirically-backed treatment option for treatment-resistant mood disorders (Parker, Roy, Hadzi-Pavlovic, & Pedi, 1992). Reduction in depressive and manic symptoms in patients following treatment has consistently been successful across a majority of populations and demographics (Ghaziuddin & Walter, 2013). However, there are populations that do not respond well to the treatment (de Vreede, Burger, & van Vliet 2005; Feske et al. 2004; Rasmussen, 2014). The proposed study is aimed at determining what demographic and personality traits predict successful treatment outcomes in adolescents and young adults receiving ECT for treatment-resistant mood disorders. Of note, those individuals with comorbid personality disorders consistently have poorer ECT treatment outcomes than those who do not have comorbid personality disorders (Rey & Walter, 1997). Personality disorders are typically diagnosed in adulthood and rarely diagnosed in adolescence given the current diagnostic criteria and potential stigma attached to the disorder (Laurenssen, Hutsebaut, Feenstra, van Busschbach, & Luyten, 2013). However, underlying personality pathologies are identifiable and present and therefore, can manifest in adverse behaviors in adolescents. Adolescents can have personality pathologies that are indicative of diagnosable personality disorders, most specifically borderline personality disorder (Ramos, Canta, de Castro, & Leal, 2014). Identifying those pathologies, some presenting externally as maladaptive behaviors, are the key to diagnosing in adolescents.
Nonsuicidal self-injury (NSSI) is the presence of self-inflicted harm without suicidal intent (American Psychiatric Association, 2013). NSSI is correlated with symptoms of personality disorders in young adults (Cawood & Huprich, 2011). NSSI has a 15.9% to 46.5% prevalence rate in high school students (Lloyd-Richardson, Perrine, Dierker, & Kelley, 2007). The high prevalence in high school students indicates a potential for different etiologies and presentations. The function(s) of NSSI is assessed and normally falls into a small number of categories: attention seeking, emotional release or relief, sense of control, self-punishment or some form of distancing self from others (Gratz, 2006; Kleindienst et al., 2008). Certain functions of NSSI may result in the self-harm becoming a repetitive cycle; there is an emotional release upon inflicting NSSI but then a significant feeling of guilt about the self-harm afterwards (Kleindienst et al., 2008). NSSI can be difficult to resolve given its potent reinforcing properties (Kool, van Meijel, & Bosman, 2009). Typically, the behavior is present with another disorder that receives precedence in treatment (e.g., major depression, generalized anxiety) and therefore, may endure following treatment.
In the proposed study, a retrospective chart review will examine roughly 70 electroconvulsive therapy Johns Hopkins Hospital patients between the ages of 13 and 25, diagnosed with a mood disorder to analyze the potential relation that the presence of NSSI has on the outcome of electroconvulsive therapy. More specifically, examining the relation between the severity of NSSI before electroconvulsive therapy to the overall change in depressive symptoms following treatment. It is hypothesized that the NSSI severity will predict a decrease in depressive symptoms. Through multiple regression, the study aims to predict the outcome depression score following ECT given the severity of NSSI and the pre-treatment depression score. In addition, patient demographic information will be examined through a one-way ANOVA to determine any moderation effects on treatment outcomes. The following describes the patient information that will be examined similar to NSSI, and its potential prediction to treatment outcomes: age, sex, race, highest level of education, Axis I and II diagnoses including personality disorder and substance abuse, family mental illness history, prior ECT treatment, psychiatric hospitalization, history of childhood abuse (emotional, physical and/or sexual), severity of NSSI, number of ECT procedures, number of ECT trials, electrode placement (i.e., right unilateral or bilateral placement or both), and concurrent medication and previous medication trials.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental
disorder-5 (5th Ed.). Washington, D.C.: Author.
Cawood, C. D., & Huprich, S. K. (2011). Late adolescent Nonsuicidal self-injury: The
roles of coping style, self-esteem, and personality pathology. Journal of Personality
Disorders, 25(6), 765-781.
Ghaziuddin, N., & Walter, G. (2013). Electroconvulsive therapy in children and adolescents. New
York, NY: Oxford University Press.
Gratz, K. (2006). Risk factors for and functions of deliberate self-harm: An empirical
and conceptual review. Clinical Psychology: Science and Practice, 10(2), 192-205.
http://dx.doi.org/10.1093/clipsy.bpg022
de Vreede, I. M., Burger, H., & van Vliet, I. M. (2005). Prediction of response to
ECT with routinely collected data in major depression. Journal of Affective Disorders,
86, 323-327. http://dx.doi.org/10.1016/j.jad.2005.03.008
Feske, U., Mulsant, B. H., Pilkonis, P. A., Soloff, P., Dolata, D., Sackeim, H. A.,
& Haskett, R. F. (2004). Clinical outcomes of ECT in patients with major depression
and comorbid borderline personality disorder. The American Journal of Psychiatry, 161(11), 2073-2080.
Kleindienst, N., Bohus, M., Ludäscher, P., Limberger, M. F., Kuenkele, K., Ebner-Priemer,
U. W., … Schmahl, C. (2008). Motives for nonsuicidal self-injury among women with
borderline personality disorder. The Journal of Nervous and Mental Disease, 196(3),
230-236. http://dx.doi.org/10.1097/NMD.0b013e3181663026
Kool, N., van Meijel, B., & Bosman, M. (2009). Behavioral change in patients with
severe self-injurious behavior: A patient’s perspective. Archives of Psychiatric Nursing,
23(1), 25- 31. http://dx.doi.org/10.1016/j.apnu.2008.02.012
Laurenssen, E. M. P., Hutsebaut, J., Feenstra, D. J., Van Busschbach, J. J., & Luyten,
P. (2013). Diagnosis of personality disorders in adolescents: A study among psychologists.
Child and Adolescent Psychiatry and Mental Health, 7, 3-7.
Lloyd-Richardson, E. E., Perrine, N., Dierker, L., & Kelley, M. L. (2007). Characteristics
and functions of non-suicidal self-injury in a community sample of adolescents.
Psychological Medicine, 37(8), 1183-1192. http://dx.doi.org/10.1017/S003329170700027X
Parker, G., Roy, K., Hadzi-Pavlovic, D., & Pedi F. (1992). Psychotic (delusional)
depression: A meta-analysis of physical treatments. Journal of Affective Disorders,
24, 17-24.
Rasmussen, K. (2014). Do patients with personality disorders respond differentially
to electroconvulsive therapy? A review of the literature and consideration of conceptual
issues. Journal of ECT, 0, 0-0.
Rey, J. M., & Walter, G. (1997). Half a century of ECT use in young people. American
Journal of Psychiatry, 154, 595-602.
Quick Details
Watch this space for more information about
the 15th annual Emerging Scholars event, planned
for April, 2026.